
The Acupuncture Profession Wants to Have Its Compassion Cake and Eat It Too
proposed revisions to ACAHM's standards and criteria

As I’ve said, everything in my world has to do double duty — including this Substack. You might have noticed I use it to organize my teaching notes (for example, what do acupuncture points do; placebo is not your enemy; a theory of gears); also, I estimate that it’s saved me approximately 1,000 internal emails for WCA and the school. Most of the time, though, I use it to think things through. I’m going to push that edge this week and try to draft a public comment for the Proposed Revisions to ACAHM’s Comprehensive Standards and Criteria.
I know, you’re probably thinking, well happy holidays to you too.

For anybody who’s sticking around for this unseasonably bureaucratic deep dive, here’s the thing — I’m having a lot of feelings about these revisions. Like, a lot. My feelings mostly don’t belong in whatever public comment I’ll eventually submit but I need to put them somewhere. That’s what blogs are for!
Let’s start with revisions for Criterion 7.04, Professional Competencies. This one takes up a lot of real estate in the document and it’s hugely important for acupuncture schools because it describes what we have to teach. 7.04 is always lit up in neon (or, okay, Christmas lights) in terms of what I pay attention to. And the revisions represent some significant changes — for example, check out Systems-Based Practice Competencies:
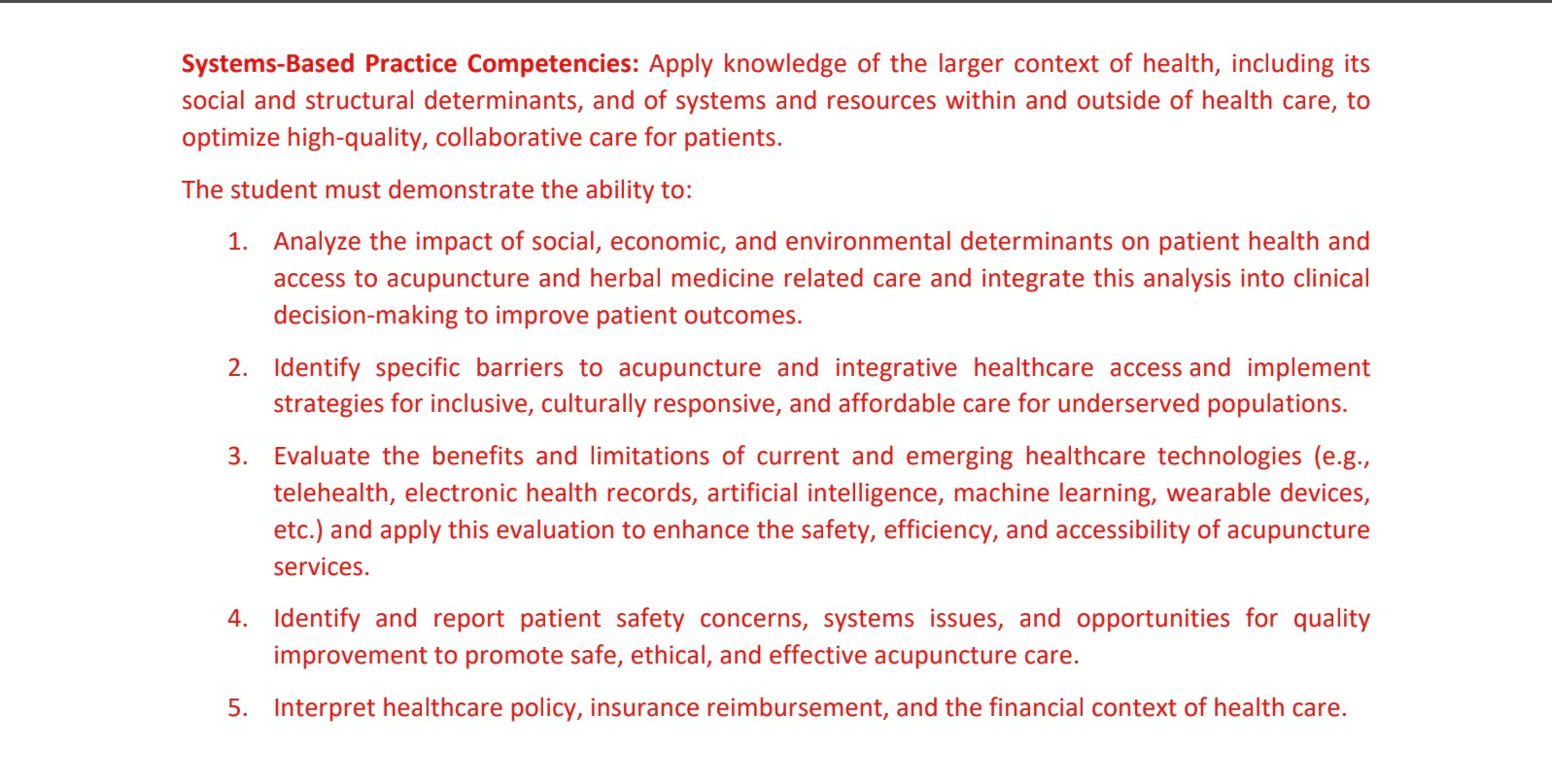
Identify specific barriers to acupuncture access and implement strategies for inclusive, culturally responsive, and affordable care for underserved populations? Am I dreaming?
For people who are new to this topic, let me summarize decades of unpleasant history by saying that the acupuncture profession and the acupuncture education industry have been treating community acupuncturists and our little school like dirt, for as long as I can remember, for doing exactly this.
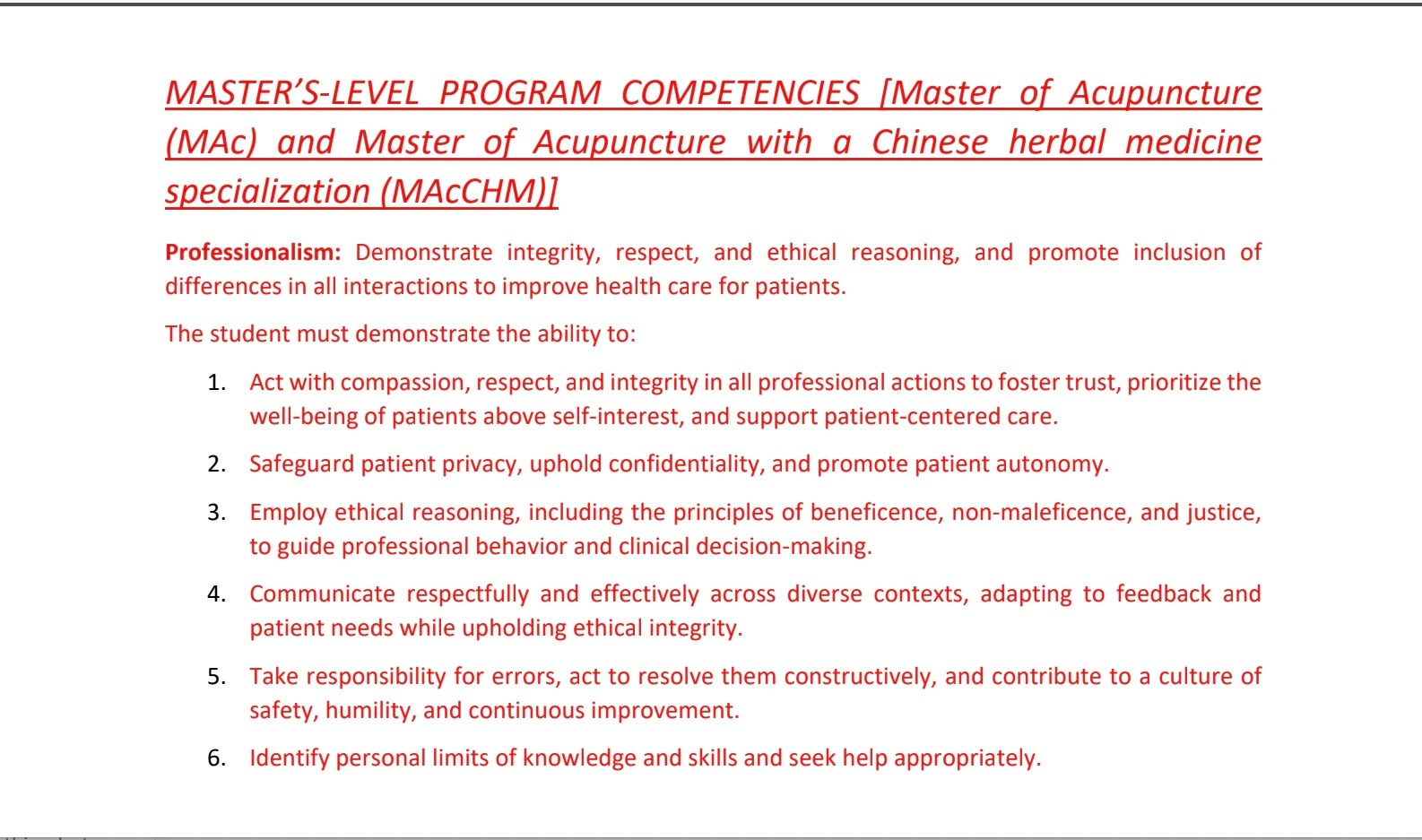
In general, the 7.04 revisions represent a sea change towards patient-centered care, patient autonomy, inclusion of differences, social determinants of health, and practitioner humility. Look at the basic definitions for professionalism and patient care:
I should be happy, right? Because this is amazing! Trauma-informed care even gets a mention later on under #10: “Deliver care that is respectful, trauma-informed, and designed to reduce health disparities.” This is our school’s whole thing. Why am I not unconditionally overjoyed about this?
I mean, on one level I’m happy (though still somewhat unbelieving). But the public comment I need to write is unfortunately a lot more complex than YAY FINALLY! THANK YOU! HO HO HO etc — because the Proposed Revisions are full of internal contradictions, thanks to the cultural and systemic biases of the acupuncture profession itself. And so while community acupuncture is suddenly being lifted up as a good example in one part of the Standards, we’re simultaneously being written into noncompliance in another part — for the same exact reasons.
Which says so much about the state of the acupuncture profession itself! Like, this particular set of contradictions is so painfully consistent and unsurprising. But still a big problem for me, so let’s proceed with unpacking it so I can write my comment.

Let’s start with the cultural bias of the acupuncture profession and the acupuncture education industry: TCM. It’s mostly unquestioned that TCM is the right way to do acupuncture and everything else is either an error or an afterthought. If you’re not teaching students to ask the 10 Questions with every patient and do differential diagnosis with every treatment, you’re doing acupuncture school wrong. If your students aren’t practicing lifestyle counseling with every patient — sorry, I mean “educating patients on behaviors that support health and self-care” — then you’re cutting corners.
That segues neatly into systemic bias: Acupuncture and integrative medicine treatments — and acupuncture education — are for middle to upper class individuals with plenty of disposable income, available time, and access to resources, who aren’t too traumatized (or too skeptical) to submit to invasive and judgemental clinical practices. That’s the target demographic, that’s who this industry is for — people who are glad to take off their clothes and be lectured to about how they should live. Any effort to modify costs, procedures, and practices to accommodate a wider diversity of patients means devaluing, degrading, and dumbing down the medicine.
Or so I’ve been hearing for the last couple of decades.
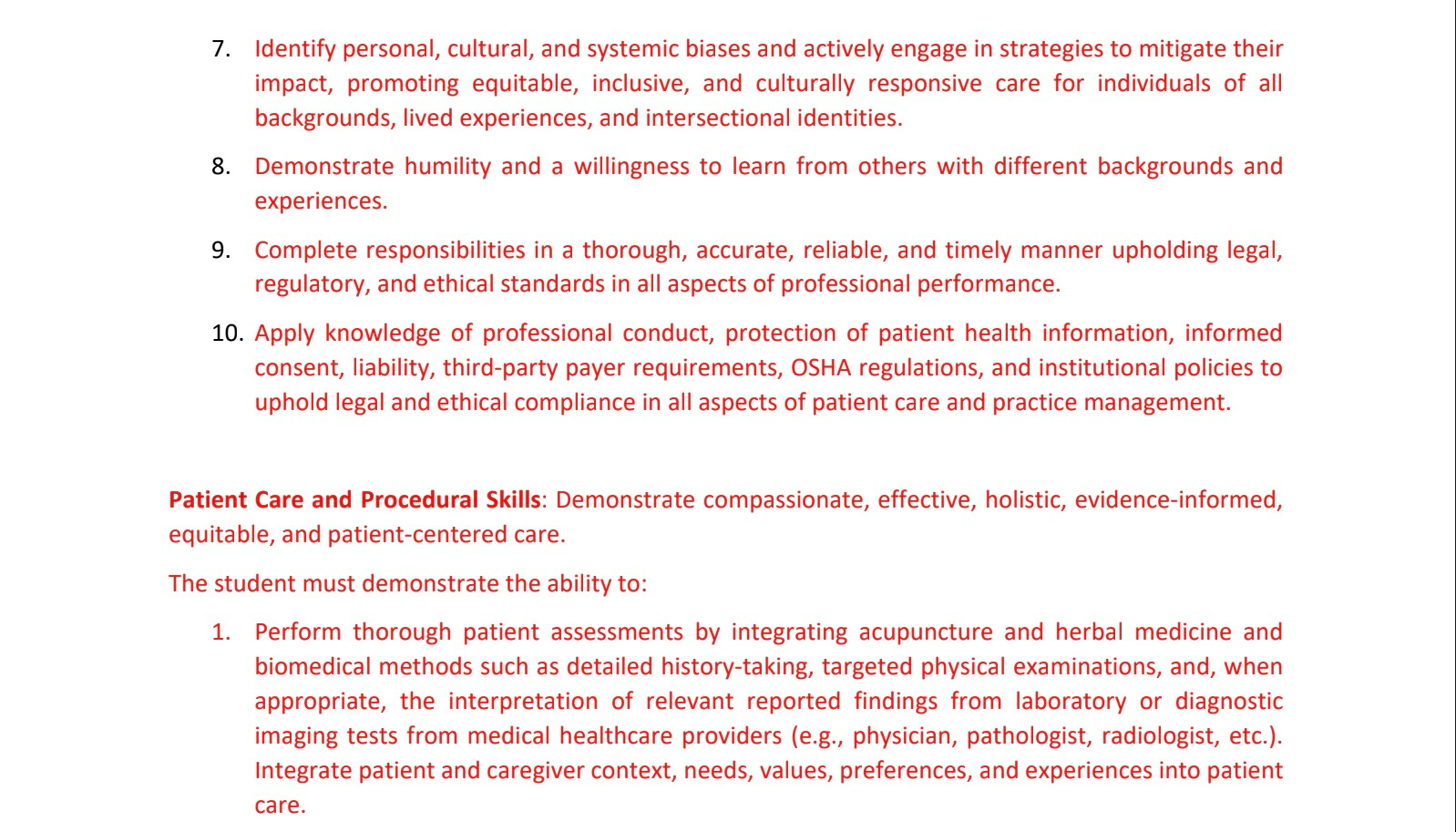
These biases are still all over the Proposed Revisions. For example, under Patient Care and Procedural Skills:
1. Perform thorough patient assessments by integrating acupuncture and herbal medicine and biomedical methods such as detailed history-taking, targeted physical examinations, and, when appropriate, the interpretation of relevant reported findings from laboratory or diagnostic imaging tests from medical healthcare providers (e.g., physician, pathologist, radiologist, etc.).
2. Accurately interpret objective and subjective findings, including laboratory, imaging, and functional assessments, to inform integrative diagnostic reasoning.
There is no actual evidence that incorporating laboratory, imaging and functional assessments results in better clinical outcomes for acupuncture treatments than not incorporating them. (Not to mention, it isn’t even legal for acupuncturists to order laboratory and imaging tests in every state.) More importantly, though, the majority of patients in our student clinics don’t have the resources to pay for this kind of intensive approach. So if we were to practice and teach this version of biomedical TCM, we’d create a “specific barrier to acupuncture access”… which is now a problem according to the Systems-Based Practice Competencies.
We’re supposed to take into account “the financial context of health care”, right? The simplest and most straightforward way to do that is to say, most community acupuncture patients can’t afford acupuncture that involves laboratory, imaging, and functional assessments — so we don’t use them, especially because there’s no evidence to support *requiring* them. But I’m confident that’s not what the acupuncture profession had in mind when these rules were being drafted. Back to this in a minute, after we talk about lifestyle counseling, which comes up a little later under Patient Care:
5. Develop, implement, and modify personalized treatment plans that reflect current clinical evidence, patient goals, and evolving conditions. Plans should integrate components of acupuncture and herbal medicine such as acupuncture, herbal medicine (MAcCHM PROGRAMS), adjunctive therapies, and lifestyle interventions to promote wellness and address disease.
The more diverse your patient base is, the more problematic it is to require “lifestyle interventions”. There’s a long list of reasons not to tell your patients what to eat, how to exercise, or how to practice, say, meditation, including: issues of access; patients’ pre-existing religious, cultural or medical restrictions around diet; the potential for triggering exercise and/or eating disorders (which can be lethal); ethical considerations around spirituality; and finally, trauma-informed care — because it’s incredibly difficult to prescribe lifestyle inventions without shaming people.
Community acupuncturists recognize that we’re mostly not treating the people who are happy to take off their clothes and be lectured to about how to live — so we just don’t do it. Because again, there’s no actual research showing that acupuncture + lifestyle counseling delivers better outcomes than acupuncture alone. Sure, some patients like lifestyle counseling and lots of acupuncturists love to do it, and that’s all (maybe) fine1 if you have a more homogeneous patient base than we do.
Lifestyle interventions are generally the enemy of inclusion. For more about this, see:
When I have to explain our clinical practices, I often use this quote from a CareOregon caseworker describing community acupuncture:
People feel welcomed at WCA. This is not always the case in the larger medical system where they may be labeled as problem patients, malingerers, drug seekers, or someone with a personality disorder. At this community acupuncture clinic, there is a predictable structure, minimal talking, and a lot of reliability which allows for relaxed and non-pressured healing relationships… By having an open door, judgments about self-care do not get in the way of treatment and, in fact, are not a part of the dialogue and culture of this clinic. This cuts down on feelings of guilt which trauma survivors so commonly battle.
This clinic asks little of patients. They don’t have to fill out forms or questionnaires every time they visit. They don’t have to share an awkward amount of personal information. For clients with trauma histories, acupuncture provides relaxation, relaxation while with other people, and access without expectation. It seems to heal the nervous system although I am not sure how. What I see with clients is not that all of their symptoms go away, but they are able to handle things in their lives better. They are able to pause; their viewpoint becomes larger. They are triggered less often and have less anxiety. Being in an environment where you are not alienated or seen as different allows peoples’ hyper-vigilance to relax. There is a major component of isolation when it comes to trauma. Community Acupuncture has the potential to heal that part of trauma.
We teach our students to ask little of patients. Because there’s an unforgiving equation that goes like this: the more you ask, the more people you exclude. If you want to promote inclusion of differences, you need to ask less.2 You need to ask people to pay less, you need to ask them to do less, and you need to modify all your systems accordingly. That’s what community acupuncture does and the acupuncture profession hates it. What we’ve been hearing for decades is, of course inclusion and access and compassion are great — but ugh, not like that.
Like what, then?
There’s an imaginary world in which acupuncturists are treating a diverse group of patients and simultaneously getting paid well by insurance for every minute of their time3, where every patient is glad to spend an hour one-on-one listening to a scholar-physician acupuncturist go over their labs and then tell them how to change their lives, and where the scholar-physician acupuncturist doesn’t have to worry about their crushing student loan debt. In that world, there are no contradictions in the Proposed Revisions. All is merry and bright.
But we don’t live in that world4 so the problem is: I think that the acupuncture profession is trying to have its compassion cake and eat it too, while they think that I’m devaluing everything with my trademark low-class style of inclusion. And now, thanks to the Proposed Revisions, that conflict is spilling all over the Standards in a way it never did before. I wonder what happens next?
In terms of the document itself, I think it’s actually pretty straightforward to resolve; it’s just a matter of writing clinical flexibility into the Standards. I won’t bore you with all the wordsmithing, but it’s probably a lot of little details like changing “Formulate prioritized pattern diagnosis and differential diagnosis using both acupuncture and herbal medical theory and biomedical frameworks” to “Formulate prioritized pattern diagnosis and/or differential diagnosis using both acupuncture and/or herbal medical theory and/or biomedical frameworks.”
However, those little adjustments would represent an even bigger sea change for the acupuncture profession: the recognition that there is no one right way to practice acupuncture (as long as you do it safely) — and so everything about acupuncture can be modified, as needed, in the service of inclusion and (truly) patient-centered care. It’s okay, you can just eat the cake.
I have a lot of questions about consent related to lifestyle counseling. I think most patients have no idea that’s what they’re signing up for when they schedule an acupuncture appointment, while acupuncturists assume it’s part of the package.
In terms of inclusion, this why 5NP is the best thing since sliced bread. (Wow, I really have a baked-goods theme going here.)
To quote Clay Daulton’s recent substack Acupuncture, Insurance and the Fever Dream: Acupuncture is a failing profession because the field has been living in a fog of aspiration for way too long.
Before anybody sends me an email that says, “But I know acupuncturists who practice inclusion and trauma informed care and they’re doing it all while giving tons of lifestyle advice and billing insurance, particularly the Oregon Health Plan”, please note that none of those acupuncturists has scaled their practice to make an accredited school. A key aspect that makes our school viable is our partnership with WCA, which is big enough to provide each cohort with between 400 and 800 treatments per intern by the time they graduate. That’s because WCA found a critical mass of people who love acupuncture but who can’t afford, or don’t want, the biomedical TCM/lifestyle advice model. If our school were required to teach and provide that model, it would wreck our student internships because WCA doesn’t do that. Our patient base depends on not doing that. No student clinic = no school. Supporting the student clinic costs WCA about $50,000 per year, give or take (because student clinics almost always lose money). If you want to try to convince those other acupuncturists to scale up their practices and make a school, so they too can lose that kind of money on training interns, have at it — but talk to them about it. Not me.
Hi Lisa – I can hardly imagine the maze of B.S. you are going through dealing with school accreditation. I want to offer a few thoughts that might help or might backfire and make you even more frustrated.
I don’t know just how much of the proposed language you quote are revisions and how that differed from the older language, but the main comments I thought to offer have to do more with the bigger picture of any Standards and Criteria for an accreditation agency in the U.S. acupuncture/CM field.
Although there is certainly the possibility of linkage, there is also a difference between the standards of what is required to be taught in accredited schools and what practitioners are expected to do in the way they practice.
These proposed standards say that “students must demonstrate the ability to:” Blah, Blah, Blah ... They do not say “these are the standards you must employ in your practice”.
The way you end up practicing is more defined by the scope of practice your license/certification allows you to do than accreditation standards. The huge problem for acupuncture/CM practice is that we have a sizable variety in scope of practice in differing states.
I know it sounds profoundly stupid that schools would be expected to teach their students KSAs they would not even be allowed to perform in some states, but this is the clusterfuck we are in trying to find the best one size fits all education standards when there is nothing close to one size fits all scope of practice standards across the various states.
An alternate route might be to allow different schools to teach different KSAs and then have multiple accreditation standards for different schools. But then, in addition to the extra complexity this would entail, what of students graduating from one school with less comprehensive/expansive Standards and Criteria based on more limited scope of practice when some of those students want to practice in a state with a broader scope?
The proposed Standards and Criteria ACAHM is proposing could make sense for a state where Acupuncturists are considered to be primary care providers (PCPs) but they go overboard for states where Acupuncturists are not PCPs. That right there is a huge freaking difference.
You and POCA Tech, with very good reason, are a proponent of a more limited training model (albeit with far more of the critical hands-on clinical training most other schools fail their students in). But if you are trying to avoid multiple training standards with all the extra complexity this would involve, you might default to justifying more expansive training as following the “better to have it and not need it than to need it and not have it” philosophy.
The same goes for the overall TCM model. Only an idiot would think that model is the only right way to practice. Even in China, that model was a compromise for the sake of uniformity and ease of regulating the practice where everyone would share a floor level knowledge and common language as the entry-level.
There was a logic behind the effort to find a one size fits all system of training that would serve as a good enough entry level education and allow practitioners to speak the same language, as it were. It should never have been seen as “the way to practice” just “the way to start to practice”. This could have been OK if we had kept the scope similar across states and adjusted the training standards to provide for that scope.
I don’t know if this was any help. Probably not. I wish I had some advice that would help your cause.
Here's the link to call for comments. I'll be weighing in (but waiting to see what Lisa has to say first!)
https://www.acahm.org/blog/proposed-revisions-to-standards